
JSER Policies
JSER Online
JSER Data
Frequency: quarterly
ISSN: 1409-6099 (Print)
ISSN: 1857-663X (Online)
Authors Info






- Read: 155463
|
ОПЦИИ ЗА ДИЈАГНОЗА И ТРЕТМАН НА АУТИСТИЧНИОТ СПЕКТАР НА НАРУШУВАЊА – ПРЕГЛЕД
Индиски институт за медицински науки, |
|
DIAGNOSTIC AND TREATMENT OPTIONS IN AUTISTIC SPECTRUM DISORDERS – AN OVERVIEW
Sheffali GULATI Biswaroop CHAKRABARTY
All India Institute of Medical Sciences, |
||
|
Примено: 29. 08. 2013 |
|
Recived: 29.08.2013 |
||
|
|
|
|
||
|
Вовед |
|
Introduction |
||
|
|
|
|
||
|
Аутизмот се карактеризира со тријада од квалитативни нарушувања во социјалните вештини, стереотипни и рестриктивни модели на интереси и искривени јазични и комуникациски вештини што се појавуваат пред 36-месечна возраст (1). Сегашната проценета преваленција на глобално ниво изнесува 1 до 2% (2). До неодамна, според Прирачникот за дијагноза и статистика за менталното нарушување (ДСМ), беше потребно нарушување во сите три домена (социјален, комуникациски и бихејвиорален) за да се дијагностицира аутизам. Сепак најновото петто издание ги спојува социјалните и комуникациските домени во еден. Исто така се препорачува под капата на терминот аутистичен спектар на нарушување да се вклучат и Аспергеров синдром, дезинтегративните растројства во детството и первазивните развојни нарушувања. Иако ДСМ V се чини дека се одликува со висока специфичност, постојат контроверзии во сензитивноста за дијагностицирање аутистичен спектар на нарушување (3). |
|
Autism is characterised by a triad of qualitative impairment of social skills, stereotypic and restrictive patterns of interests and defective language and communication skills with onset before 36 months of age (1). The current estimated global prevalence rate is 1 to 2% (2). Until recently the Diagnostic and Statistical Manual of Mental Disorders (DSM) required impairment in all 3 domains (social, communication and behavioural) to diagnose autism; however, the most recent and 5th edition have merged the social and communication domains into one. It has also been recommended to include Asperger’s syndrome, childhood disintegrative disorder and pervasive developmental disorder all under the umbrella term of autistic spectrum disorder. Although DSM V seems to have high specificity, controversy exists with its sensitivity for diagnosing autistic spectrum disorder (3). |
||
|
|
|
|
||
Дијагностицирање аутизам |
|
Diagnosis of autism |
||
|
|
|
|
||
|
Според критериумите на ДСМ V, потребно е исполнување на сите 3 симптоми во социјалната интеракција и најмалку два симптома во доменот на репетитивното однесување. Сепак, се смета дека тоа се многу строги критериуми во споредба со ДСМ IV. Постои веројатност дека ПРН – НДН (первазивни развојни нарушувања, неспецифицирани на друг начин) се испуштаат, како и високо функционирачки аутизам, вклучувајќи го и Аспергеровиот синдром (3). Медицинските евалуации се фокусираат на генетското тестирање, невровизуелизацијата, електроенцефалографијата и метаболичкиот скрининг (Слика 1). Лабораториските истражувања не се рутински индицирани и разгледувани на индивидуална основа (7) |
|
The DSM V criteria require fulfillment of all 3 symptoms in social interaction and communication domain and at least 2 symptoms in repetitive behavioural domain. However, it comes across as very stringent diagnostic criteria compared to DSM IV. There is a high probability of missing out PDD-NOS (pervasive developmental disorders, not otherwise specified) and high functioning autistics including Asperger’s Syndrome (3). Medical evaluation focuses on genetic testing, neuroimaging, electroencephalography and metabolic screening (Figure 1). Laboratory investigations are not routinely indicated and considered on an individual basis (7) |
||
|
|
||||
|
|
||||
|
Слика 1: Истражувачки пристап на аутизмот |
|
Figure 1: Investigational approach to autism |
||
|
|
|
|
||
|
Генетско тестирање |
|
Genetic testing |
||
|
|
|
|
||
|
Американската академија за педијатрија (ААП) ја препорачува хромозомската анализа за сите аутистични деца. Сепак, за општите синдроми, (Фрагилен Х и Ретов синдром), препорачани се посебни генетски студии. Кариотипот се препорачува доколку постои сомнеж за балансирана транслокација (≥2 спонтани абортуса). Индивидуите со голема глава треба да бидат изложени на ПТЕН-анализа за мутација (9). |
|
American Academy of Pediatrics (AAP) recommends chromosomal microarray analysis for all autistic children. However, for common syndromes (Fragile X and Rett) specific genetic studies are recommended. Karyotype is advocated if a balanced translocation (≥ 2 miscarriages) is suspected. Macrocephalic individuals should be subjected to PTEN mutation analysis (9). |
||
|
|
|
|
||
|
Невровизуализација |
|
Neuroimaging |
||
|
|
|
|
||
|
Магнетна резонанца се препорачува за пациенти со микроцефалија, акутно заостанување, невромалигни маркери, аномалии на лице и абнормални невролошки испитувања (10). |
|
A Brain MRI is indicated for patients with microcephaly, acute regression, neurocutaneous markers, midline facial anomalies and abnormal neurological examination (10). |
||
|
|
|
|
||
|
Електроенцефалографија |
|
Electroencephalography |
||
|
|
|
|
||
|
Електроенцефалографија се препорачува за пациенти со акутно заостанување, необјаснета енцефалопатија или промени во однесувањето, клинички напади или сомнителни субклинички напади (9, 10). |
|
Electroencephalography is recommended in patients with acute regression, unexplained encephalopathy or behavioural changes, clinical seizures or suspected subclinical seizures (9, 10). |
||
|
|
|
|
||
|
Метаболни студии |
|
Metabolic studies |
||
|
|
|
|
||
|
Според ААП, треба да се провери нивото на артериските лактати, пирувати, нивоата на крвниот карнитин и ацилкарнитин, уринарните органски и аминокиселини, функцијата на црниот дроб и бубрезите доколку постои повраќање, хипотонија, апатија со болест што се јавува меѓувремено, абнормална миризба на телесните течности, мултиорганско вклучување, дисморфизам и нарушување на движењето. Оние што јадат земја, песок, треба да се подложат на тестирање на нивото на олово, додека тестирање на железото може да се направи кај сите (9, 10). Во студијата на Sehgal и cop. од Индија не била најдена поврзаност на нивото на тешки метали во серумот (олово и жива) и симптоми кај аутистичните деца (11). |
|
According to AAP, arterial lactate, pyruvate, blood carnitine and acylcarnitine levels, urine organic and aminoacids, liver and renal function tests should be done in cases with cyclical vomiting, hypotonia, letharginess with intercurrent illnesses, abnormal odour of body fluids, multiorgan involvement, dysmorphism and movement disorder. Those with associated pica should undergo lead level testing, whereas iron studies can be done in all (9, 10). In a study by Sehgal et al. from India, no correlation was found between serum levels of heavy metals (lead and mercury) and symptoms in autistic children (11). |
||
|
|
|
|
||
|
Можности за третман |
|
Treatment options |
||
|
|
|
|
||
|
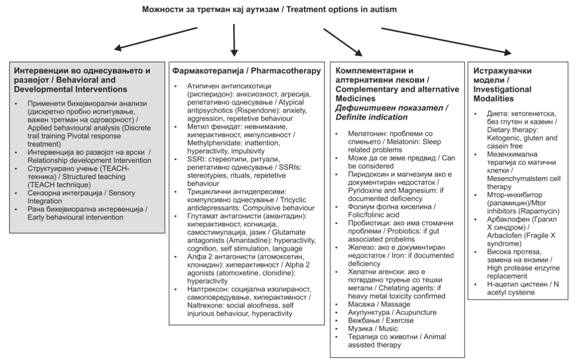
Најважни се бихејвиоралните интервенции (9, 12). Одредени карактеристики можат да се контролираат со фармакотерапија. Разни други начини на терапија, вклучувајќи ја и промената на начинот на исхрана, моментално се испитуваат (слика 2). |
|
The mainstay is behavioural intervention (9, 12). Certain features are amenable to control by pharmacotherapy. Various other modes of therapies, including dietary modifications, are currently under investigation (figure 2). |
||
|
|
||||
|
Слика 2: Можности за третман на аутизам |
|
Figure 2: Treatment options in autism |
||
|
|
|
|
||
|
Психосоцијални интервенции |
|
Psychosocial interventions |
||
|
|
|
|
||
|
Разни начини на бихејвиорална и развојна интервенција се развиени за главните проблеми на аутизмот. Сепак, моментално не постои ниту еден алгоритам базиран на докази. Примената зависи од самиот пациент (9, 12). |
|
Various behavioural and developmental intervention models have been developed for the core issues of autism. However currently there is no single evidence based algorithm. Application is individual patient based (9, 12). |
||
|
|
|
|
||
|
Применета бихејвиорална анализа (ПБА) |
|
Applied behavioural analysis (ABA) |
||
|
|
|
|
||
|
Ова е спроведено во структурирана средина преку зајакната техника на учење. Дискретно пробно испитување (ДПИ, популарно како техника на Ловас, развиена на Универзитетот во Калифорнија) е најчесто употребувана форма од овој метод. Акцентот е на основните вештини, како внимание, усогласување, имитација и постапно учење на мали индивидуални задачи. Документирани се значителни подобрувања во когнитивното однесување, јазичните и социјалните вештини (9, 13, 14). Раната интензивна интервенција на однесувањето (РИИО) е посебна форма на интервенција што се применува 20 до 40 часа неделно. Cochrane ја прикажува како ефективен модел, но сепак се препорачуваат рандомизирани испитувања за подефинитивни заклучоци (15). Се појавил уникатен модел на бихејвиоралната интервенција базирана на бихејвиорална анализа преку активности на игра, наречени ран Денверов модел, кој покажал ефикасност кај деца од 12 до 18 месеци кај рандомизирани клинички испитувања (16). |
|
This is conducted in a structured environment through reinforcement learning technique. Discrete trial training (DTT, popularly known as Lovaas technique, developed at the University of California) is the most practised form of this method. The stress is on basic skills like attention, compliance, imitation and breaking down learning into small individual tasks. Significant improvements in cognition, adaptive behaviour, language and social skills have been documented (9, 13, 14). Early Intensive Behavioural Intervention (EIBI) is a specific form of this intervention given for 20 to 40 hours per week. Cochrane has shown it as an effective modality; however, further randomized trials are recommended for more definite conclusions (15). A unique model of behavioural intervention based on applied behavioural analysis through play activities called Early Denver Model has emerged, which has shown effectiveness in children aged 12 to 18 months in randomised controlled trials (16). |
||
|
|
|
|
||
|
Развојни пристапи |
|
Developmental approaches |
||
|
|
|
|
||
|
Истражуван е модел базиран на развојните индивидуални разлики во односите интегриран со игра на под. Возрасните се вклучуваат во игра со децата на под и го стимулираат учењето во социјални и емоционални сфери. Рандомизираните испитувања покажуваат значително подобрување на социјалните вештини при интервенција (20, 21). Интервенцијата за развој на врските (ИРВ) се базира на концептот на динамична интелигенција или флексибилно размислување (22, 23). ТЦР ги комбинира и бихејвиоралниот и развојниот пристап. |
|
A developmental individual difference relationship based (DIR) model integrated with floor play is being evaluated. Adults engage in floor play with children and stimulate learning in social and emotional spheres. Randomised trials have documented significant improvement in social skills in the intervention arm (20, 21). Relationship development intervention (RDI) is based on the concept of dynamic intelligence or flexible thinking (22, 23). PRT combines both behavioural and developmental approaches. |
||
|
|
|
|
||
|
Структурирано учење |
|
Structured teaching |
||
|
|
|
|
||
|
Популарно познатиот TEACHH-модел (тренинг и подучување на аутистични деца и деца со тешкотии во комуникацијата) истакнува модифицирање на средината на детето според неговиот недостаток и неговите потреби. Ова е еклектичен пристап на тренинг што се спроведува во организирана физичка средина преку визуелно структуирана активност и распореди што истакнуваат неколку можности на кои може да се заврши одредена задача (17, 24). |
|
Popularly known as the TEACHH (training and education of autistic and related communication handicapped children) model, it emphasizes modifying the child’s environment according to his deficits and needs. This is an eclectic approach of training done in an organized physical environment through visually structured activity and schedules, emphasising several options by which a particular work can be done (17, 24). |
||
|
|
|
|
||
|
Сензорна интеграција |
|
Sensory Integration |
||
|
|
|
|
||
|
Се претпоставува дека аутистичните деца се хипо или хиперсензитивни на сензорни информации, што се манифестира како нарушена способност да се интерпретираат вестибуларни, проприоцептивни и тактилни стимулуси. Идеална сензорна интеграција се овозможува преку активности како тресење, скокање, клацкање и лулање. Се користат различни техники, виз., силен притисок, заедничка компресија, триење на тело, орално-моторни вежби и говор на тело (25). Сепак, ова е концепт што се развива и потребни се повеќе студии за да се потврди неговата полза. |
|
Autistic children are presumed to be hypo or hypersensitive to sensory input which manifests as impaired ability to interpret and act on vestibular, proprioceptive or tactile stimuli. Ideally sensory integration is provided in activities like rocking, jumping, swinging and rolling. Various techniques are used, viz., deep pressure, joint compression, body brushing, weighted vests, oral-motor exercises and body massage (25). However this is an evolving concept and more studies are required to validate its utility. |
||
|
|
|
|
||
|
Рани бихејвиорални интервенции |
|
Early behavioural intervention |
||
|
|
|
|
||
|
Одредени знаци кај новороденчиња и мали деца можат да го предвидат појавувањето на аутизам, сепак потребно е понатамошно истражување за целосно објаснување. Ова опфаќа намалено гугање и нарушено социјално реагирање со тешкотии во гестикуларната комуникација, нарушено внимание и имитирање и слаба реакција на името, коишто се од поран датум (26). Во моментот, се евалуира раниот Денверов модел кај новороденчиња на возраст од 6 месеци кај кои постојат знаци за појава на ран аутизам (9). |
|
Certain clinical pointers in infants and early toddler group can predict future occurrence of autism; however, further research is needed for complete delineation. These include reduced babbling and impaired social responsiveness predated by difficulty in gestural communication, impaired joint attention and imitation and poor response to name (26). Currently, Early Denver model is being evaluated in infants as young as 6 months with features of suspected early autism (9). |
||
|
|
|
|
||
|
Фармакотерапија |
|
Pharmacotherapy |
||
|
|
|
|
||
|
Не постои одобрена фармакотерапија за главните симптоми за аутизам, сепак можат да се користат лекови за да се намалат бихејвиоралните проблеми, како хиперактивност, невнимание, агресија, несоница, самоповредување и вознемиреност. Одлуката да се започне со фармакотерапија што ќе се базира на индивидуални случаи и ќе се одреди по бихејвиорална интервенција по одреден период, не покажа значајно подобрување. Со постојаната терапија со лекови треба да продолжат и бихејвиоралните интервенции. |
|
There is no FDA approved pharmacotherapy for core symptoms of autism; however, drugs may be used to ameliorate behavioural problems like hyperactivity, inattention, aggression, insomnia, self injury and anxiety. Decision to initiate pharmacotherapy that should be based on the individual case and done only after behavioural intervention over a significant period of time, has not shown much improvement. With ongoing drug therapy behavioural interventions should continue. |
||
|
|
|
|
||
|
Нетипични антипсихотици |
|
Atypical antipsychotics |
||
|
|
|
|
||
|
Рисперидон и арипипразол се единствените два лека што се одобрени од ФДА за третирање раздразливост кај аутистични деца. Откриено е дека рисперидонот ја намалува возбудата, агресијата и репетитивното однесување. Забележани се повремена поспаност и зголемување на телесната тежина. Респеридонот има и антиоксидативни и неврозаштитни ефекти (27, 28). |
|
Risperidone and aripiprazole are the only two FDA approved drugs for treating irritability in autistic children. Risperidone has been found to reduce anxiety, aggression and repetitive behaviour. Occasionally sedation and weight gain has been reported. Risperidone also possesses antioxidant and neuroprotective effects (27, 28). |
||
|
|
|
|
||
|
Метилфенидат |
|
Methylphenidate |
||
|
|
|
|
||
|
Ефикасен е за невнимание, хиперактивност и импулсивност. Сепак, треба да се внимава на несаканите ефекти, како несоница, анорексија и промени на расположението. Исто така забележан е и забавен раст при долготрајна употреба (29). |
|
It is effective for inattention, hyperactivity and impulsivity. However, one has to be cautious about side effects like sleeplessness, anorexia and mood swings. Growth failure has also been documented with prolonged use (29). |
||
|
|
|
|
||
|
Селективни серотонински повратни инхибитори |
|
Selective Serotonin Reuptake inhibitors |
||
|
|
|
|
||
|
Флуоксетинот и сличните лекови се корисни за намалување на стереотипното, ритуалното и репетитивното однесување. Сепак, треба да се внимава на несаканите ефекти, како дезинхибиција, хипоманија и хиперактивност (28). |
|
Flixetine and its congeners are beneficial in reducing stereotypies, rituals and repetitive behavior. However, side effects like disinhibition, hypomania and hyperactivity are to be watched for (28). |
||
|
|
|
|
||
|
Трициклични антидепресиви |
|
Tricyclic Antidepressants |
||
|
|
|
|
||
|
Во споредба со плацебо во рандомизирано клиничко испитување, кломипраминот и десипраминот покажале значително подобрување на компулсивното однесување. Сепак, забележани се несакани ефекти како агресија и хиперактивност (28, 30). |
|
Compared to placebo in a randomized controlled trial, clomipramine and desipramine have shown significant improvement in compulsive behaviours. However side effects like aggression and hyperactivity have been described (28, 30). |
||
|
|
|
|
||
|
Антиепилептици |
|
Antiepileptics |
||
|
|
|
|
||
|
Леветирецетам и валпроат покажуваат ефикасност за намалување на симптомите како хиперактивност, агресија, нарушени социјални вештини, афективна нестабилност кај неепилептични аутистични деца (28, 31). |
|
Levetirecetam and valproate have shown effectiveness in reducing symptoms like hyperactivity, aggression, impaired social skills and affective instability in non-epileptic autistic children (28, 31). |
||
|
|
|
|
||
|
Глутамат антагонисти |
|
Glutamate antagonists |
||
|
|
|
|
||
|
Еден од постулираните механизми на аутистичната патогенеза е глутамат ексцитотоксичност. Истражувањата покажаа подобрување кај хиперактивноста, когницијата, јазичните проблеми и самостимулацијата со глутаматните антагонисти амантадин и мемантин (32, 33). |
|
One of the postulated mechanisms of autism pathogenesis is glutamate excitotoxicity. Studies have shown improvement in hyperactivity, cognition, language problems and self stimulation with glutamate antagonists amantadine and memantine (32, 33). |
||
|
|
|
|
||
|
Ацетилхолинестеразни инхибитори |
|
Acetylcholinesterase inhibitors |
||
|
|
|
|
||
|
Лековите како донепезил и галантамин го намалуваат аутистичното однесување, раздразливоста и хиперактивноста, но сепак треба да се биде внимателен за холинергичните несакани ефекти (28, 34) |
|
Drugs like Donepezil and Galantamine reduce overall autistic behavior, irritability and hyper activity; however, one has to be vigilant for the cholinergic side effects (28, 34). |
||
|
|
|
|
||
|
Алфа – 2 агонисти |
|
Alpha- 2 agonists |
||
|
|
|
|
||
|
Атомоксетин и клонидин се добро толерантни селективни антагонисти, кои ја подобруваат хиперактивноста, промените на расположението, агресијата и спиењето кај пациенти со аутистичен спектар на нарушувања (9, 35) |
|
Atomoxetine and Clonidine are well tolerated selective α-2 agonists, which improve hyperactivity, mood swings, aggression and sleep architecture in patients with autistic spectrum disorder (9, 35). |
||
|
|
|
|
||
|
Опиодни антагонисти |
|
Opioid antagonist |
||
|
|
|
|
||
|
Ендогените опиоди како ендорфините и енкефалините го регулираат социјалното однесување. Неколку студии покажале дека опиодните антагонисти, како налтрексон, можат да доведат до намалување на самоповредувањето, хиперактивноста и социјалното повлекување (36). |
|
Endogenous opioids like endorphins and enkephalins regulate social behaviour. Few studies have shown that opioid antagonists like Naltrexone can lead to improvement in self-injurious behaviour, hyperactivity and social aloofness (36). |
||
|
|
|
|
||
|
Комплементарни и алтернативни третмани |
|
Complementary and alternate treatments |
||
|
|
|
|
||
|
Ова е група на разни алтернативни медицински и здравствени системи, практики и производи што генерално не се земаат како дел од конвенционалната медицина. Тие се дополнителни кога се применуваат заедно со конвенционалната медицина и алтернативни кога се користат сами. До ¾ од пациентите со аутизам се изложени на алтернативни или комплементарни третмани. Досега не постојат дефинитивни можости за лекување; со користење на овие методи се очекува плацебо ефект бидејќи тие се достапни, помалку галопирачки и психолошки поутешителни за родителите. Сепак, дететето со здравствени ризици не треба да се изложува на други ефективни терапии, а семејството да се изложува на дополнителен финансиски трошок (9, 37). |
|
These are group of diverse medical and health care systems, practices and products that are generally not considered part of conventional medicine. They are complementary when used along with conventional medicines and alternate when they are used alone. Upto ¾ of the patients with autism undergo some form of alternate or complementary treatment. As of currently, there are no definite curative options available, a placebo effect is expected with these modalities as they are accessible, less invasive and psychologically more comforting for the parents. However, it should not present the child with health risks, be detrimental towards other effective therapies and cause undue financial burden to the family (9, 37). |
||
|
|
|
|
||
|
Мелатонин
Витамин Б6 и магнезиум
Фолна киселина
Омега 3 масни киселини
Пробиотици
Железо
Агенси за хелација
Л-карнозин |
|
Melatonin
Vitamin B6 and Magnesium
Folic acid
Omega3 fatty acids
Probiotics
Iron
Chelating agents
L-Carnosine |
||
|
|
|
|
||
|
Терапија со исхрана |
|
Dietary therapies |
||
|
|
|
|
||
|
Се проценува дека исхраната без глутен и казеин, како и кетоисхраната, во мал степен помагаат на аутистичните деца. Се претпоставува дека глутенски и казеински поврзаните пептиди можат да придонесат за патогенезата на аутизмот, предизвикувајќи зголемена опиоидна активност. Сепак, не постојат докази кои ја фаворизираат нивната примена и препорачани се подобро дизајнирани студии (46). Среден синџир на триглицеридна кетоисхрана покажува значително подобрување на бихејвиоралните проблеми поврзани со аутизмот. Се претпоставува дека невромодулацијата посредувана од аденозин е основен механизам. Сепак, резултатите треба да се проверат во поголеми лонгитудални студии (47). |
|
Both gluten and casein free and ketogenic diet have been evaluated in a small scale for autistic children. It has been hypothesized that gluten and casein related peptides may contribute to the pathogenesis of autism by stimulating excessive opioid activity. However, currently there is no definite evidence favouring their use and well designed studies are recommended (46). A medium chain triglyceride based ketogenic diet has shown significant improvement in the behavioural issues associated with autism. Adenosine mediated neuromodulation has been postulated to be the underlying mechanism. However, the results need to be replicated in larger longitudinal studies (47). |
||
|
|
|
|
||
|
Терапија со матични клетки |
|
Stem cell therapy |
||
|
|
|
|
||
|
Аутистичниот мозок се карактеризира со церебеларни промени, како намалени Пуркиниеви клетки, дефектна организација на мозочната кора, абнормална пластичност на морфологијата на ’рбетниот мозок. Се претпоставува дека мезенхималните матични клетки можат да ги обноват церебеларните Пуркиниеви клетки, да ја зајакнат и да ја закрепнат кортикалната и синаптичката пластичност. Како и да е, многу прашања се неодговорени, како, на пример, контроверзијата за употребата на егзогените или ендогените матични клетки, недостатокот во чување на долготрајна меморија и претклиничките испитувања (48). |
|
An autistic brain is characterized by cerebellar alterations like decreased purkinje cells, defective cortical organization and aberrant plasticity of dendritic spine morphology. It has been hypothesized that mesenchymal stem cells may restore cerebellar purkinje cells, reinforce and promote cortical and synaptic plasticity. However there are various unanswered questions, like, controversy regarding use of exogenous or endogenous stem cells, lack of long term safety data and preclinical studies (48). |
||
|
|
|
|
||
|
Модели на третман при испитување на mTOR (mammalian target of rapamycin)инхибитори |
|
Treatment modalities under investigation |
||
|
|
|
|
||
|
Дезинхибиција на mTOR сигнализирањето е забележано во различни генетски модели на аутизам (туберозна склероза, неврофиброматоза и Фрагилен Х-синдром). МТОR-инхибиторите како рапамицин се вреднуваат особено во туберозната склероза во однос на подобрување на разбирањето, однесувањето и невролошките симптоми (49). |
|
Disinhibited mTOR signaling has been documented in various genetic models of autism (tuberous sclerosis, neurofibromatosis and fragile X syndrome). MTOR inhibitors like rapamycin are being evaluated particularly in tuberous sclerosis in terms of improvement in cognition, behaviour and neurological symptoms (49). |
||
|
|
|
|
||
|
Арбаклофен кај Фрагилен Х-синдромот |
|
Arbaclofen in Fragile X syndrome |
||
|
|
|
|
||
|
Арбаклофенот (ГАБАб агонист) се вреднува во пилот студија што вклучува пациенти со Фрагилен Х-синдром кои покажуваат подобрување на невробихејвиоралното функционирање (9). |
|
Arbaclofen (GABAb agonist) has been evaluated in a pilot study involving fragile X syndrome patients showing improvement in neurobehavioural functioning (9). |
||
|
|
|
|
||
|
Конфликт на интереси Авторите изјавуваат дека немаат конфликт на интереси. |
|
Conflict of interests Authors declare no conflict of interests. |
||
|
Citation: Gulati S, Chakrabarty B. Diagnostic and Treatment Options in Autistic Spectrum Didorders – an Overview. J Spec Educ Rehab 2014; 15(1-2):43-58. doi: 10.2478/JSER-2014-0003 |
||||
|
Article Level Metrics |
||||
.jpg)
|
|
|
|
Follow Us
Share Us
Journal metrics
-
 SNIP 0.059
SNIP 0.059 -
IPP 0.07
-
 SJR 0.13
SJR 0.13 -
 h5-index 7
h5-index 7 -
 Google-based impact factor: 0.68
Google-based impact factor: 0.68
Related Articles
Indexed in




![]()
10 Most Read Articles
- PARENTAL ACCEPTANCE / REJECTION AND EMOTIONAL INTELLIGENCE AMONG ADOLESCENTS WITH AND WITHOUT DELINQUENT BEHAVIOR
- RELATIONSHIP BETWEEN LIFE BUILDING SKILLS AND SOCIAL ADJUSTMENT OF STUDENTS WITH HEARING IMPAIRMENT: IMPLICATIONS FOR COUNSELING
- EXPERIENCES FROM THE EDUCATIONAL SYSTEM – NARRATIVES OF PARENTS WITH CHILDREN WITH DISABILITIES IN CROATIA
- INOVATIONS IN THERAPY OF AUTISM
- DIAGNOSTIC AND TREATMENT OPTIONS IN AUTISTIC SPECTRUM DISORDERS – AN OVERVIEW
- AUTISM AND TUBEROUS SCLEROSIS
- REVIEW OF SPECIAL EDUCATION PROGRAMS IN JORDAN: CURRENT PRACTICES, CHALLENGES, AND PROSPECTS
- THE DURATION AND PHASES OF QUALITATIVE RESEARCH
- REHABILITATION OF PERSONS WITH CEREBRAL PALSY
- DISORDERED ATTENTION AS NEUROPSYCHOLOGICAL COGNITIVE DISFUNCTION